
Upon first seeing
their MRIs, many people with spinal-cord injury (SCI) have said to
themselves, "But everything below my injury can't be paralyzed!
There's barely a notch in my spinal cord!"
Perhaps SCI’s
cruelest aspect is its uncertainty. We wonder how our bodies could
become so impaired through so little apparent damage, whether its lost
functions might one day return, and what types of repairs are needed to
regain them.
Since the 1970s, a
passive neuromuscular training technique developed by Dr. Bernard
Brucker, University of Miami, called the Brucker Biofeedback Method, has
allowed many with SCI to regain functional abilities. 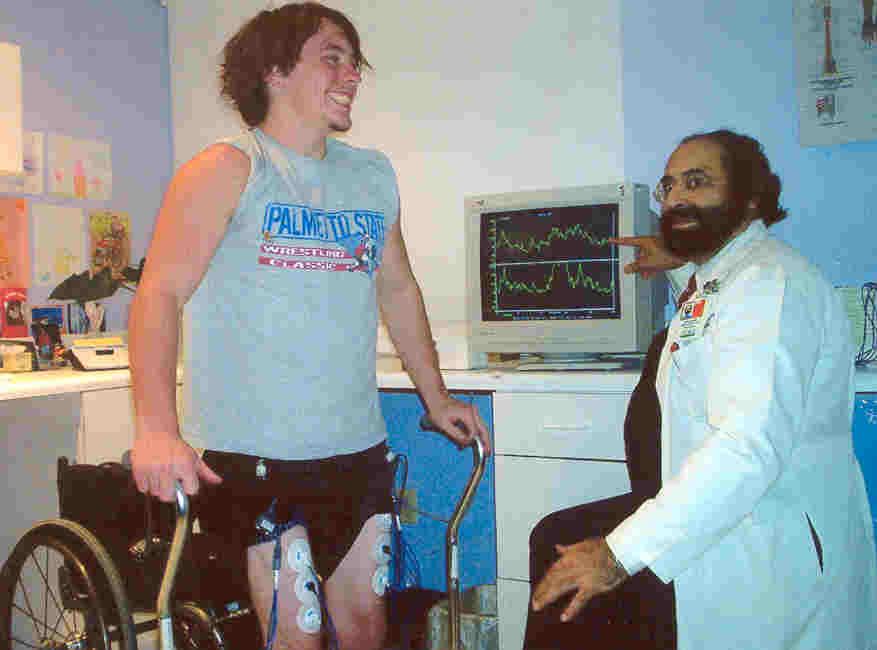
This method uses
visual “feedback” from an
electromyography (EMG) device. Through sensitive electrodes placed over
muscles, EMGs sense motor-action potentials (nerve “impulses” or
signals) with great precision. The EMG visual display allows users and
therapists to “see” subtle neural signals that reach the muscles from
the brain, which the user is unable to sense. Seeing these signals
enables trained therapists to choose specific rehabilitative techniques
aimed at strengthening the signals until they produce a desired
functional effect, e.g., the user can voluntarily contract a previously
paralyzed muscle.
This technique has
improved the quality of life for many with SCI
by shedding light on one of its
previously uncertain aspects: the cord's functional potential in its
chronically injured state. However, as reparative treatments for chronic
SCI move from the lab to the clinic, biofeedback’s benefits to the
paralyzed community may broaden far beyond its present uses; they may be
integral to emerging regenerative successes.
This two-part
article explores biofeedback’s proven benefits and future potentials.
How
Biofeedback “Works”
Biofeedback is a
form of operant learning, which uses a “reinforced stimulus” as a reward
to encourage the subject to repeat a desired action. During biofeedback,
the patient is requested to perform intended movements. Using a movable
graph on a computer screen, the EMG provides visual feedback of neural
signals that reach target muscles. The subject may need repeated
attempts to “find” a neural pathway that delivers a signal. But even
then the signal is often too weak for the subject to sense.
Once a pathway is found, the therapist directs
the subject to make the EMG graph “grow.” This can only occur by
increasing the strength of the motor signal that reaches the muscle.
However, because the subject may not sense the signal, or signal
variations may be too slight to be felt at first, EMG feedback is used
to provide the “reinforced stimulus” necessary for operant learning to
occur.
By teaching subjects how to reproduce, maintain
and control EMG responses for maximum improvements in muscle function,
EMG visual feedback – combined with behavioral conditioning techniques
and rehabilitation – helps subjects “re-educate” their muscles. The
control gained in one session is the starting point for the next.
SCI
Applications
The Brucker
Technique uses the Neuroeducator 3 EMG Biofeedback System, which allows
therapists to identity subtle motor connections between the brain and
the body that survived injury, or that have slowly repaired or rebuilt
since being damaged.
Unlike biofeedback
to enhance relaxation, control blood pressure, or control heart rate,
SCI biofeedback requires equipment sensitive enough to monitor neural
signals to within 1% of normal signal. In addition, biofeedback-trained
therapists should know which muscles are needed to regain specific motor
functions, the signal strength needed for specific muscles to function,
and techniques for helping the subject find and develop these signals.
Subjects with SCI
have regained many lost motor functions after biofeedback training. The
results sometimes appear as miraculous. People who were told that they
would never walk or use their hands have regained the ability to walk or
feed themselves. However, motor improvements through biofeedback therapy
require the patient to have specific physical conditions.
Q & A
Dr. Bernard Brucker,
founder and an original co-director of the Miami Project to Cure
Paralysis, currently directs the University of Miami School of
Medicine’s Biofeedback Laboratory.
JPK:
How soon can the therapist know if improvements are possible?
Dr. Brucker:
A biofeedback therapist can tell during the first treatment whether
neural connections exist for each muscle tested. The likelihood of
functional improvements depends on the strength of motor signals that
reach the muscles. For example, the quadriceps require roughly 14%
normal motor signal to trigger voluntary contractions. If 10% reaches
the muscle when the subject first attempts to move it, experience
suggests that the movement threshold might be reached in the first or
second session. More sessions are needed if the initial signal is lower,
but still strong enough to imply that a muscle’s functional threshold
might be reached.
JPK:
Does injury level or neurological “completeness” limit potential
benefits?
Dr. B:
Biofeedback therapy can lead to functional improvements regardless of
injury level or completeness. Moreover, MRIs are unable to accurately
predict biofeedback outcomes, because they are unable to determine
neural conductivity. Subjects with injuries evaluated as complete have
made substantial improvements through biofeedback. Whereas others with
slight-to-moderate incomplete SCI have improved only slightly. It is
rare that biofeedback fails to exert some benefits.
JPK:
Does time post injury affect biofeedback’s possible effects?
Dr. B: Efficacy
can be affected by time post injury for the good or bad. Patients
who had little neural sparing (through the injury site) soon after
injury might have considerable disused connections ready to be found and
used, once enough time elapses to permit neural repairs, or remodeling.
However, too much time post injury can contribute to muscle atrophy,
contractures, and bone-density loss, which all adversely affect an
individual’s ability to benefit from biofeedback.
JPK:
How much improvement is typically seen?
Dr. B:
Roughly 98% of individuals with SCI who undergo biofeedback improve at
least one vertebra level of functionality. Therefore the condition of an
individual with C-7 injury might improve to that generally found in
those with T-1 injuries. Ninety-five percent improve two functional
levels, and 85% improve three. Greater improvements are too erratic to
predict. However, improvements may occur in functions controlled by
nerves that leave the cord far below the lesion before being seen in
functions controlled by nerves that leave the cord just below the injury
site.
JPK:
Can biofeedback lead to other benefits?
Dr. B:
Biofeedback can have positive effects on urinary incontinence, bowel
control, respiratory functions, and spasticity. It is ineffective for
treating chronic pain. Improved muscle tone and control of abdominal
muscles can indirectly improve bowel and bladder control. Spasticity
often decreases when improvements are made in voluntary motor signal
strength. Previously ventilator-dependant subjects have improved the use
of intercostal muscles, which assists upper-chest-cavity breathing (as
opposed to diaphragmatic breathing).
JPK:
How many sessions are needed to achieve maximum results?
Dr. B:
Fifteen sessions are normally advised.
JPK:
Are follow-up treatments indicated once improvements plateau?
Dr. B: At
this point,
further therapy is unlikely to lead to additional gains. However,
because neural repairs in the cord can slowly occur over time, periodic
biofeedback evaluation may reveal new potential for improvement.
Conclusion:
Although the Brucker
Biofeedback Method has improved the lives of many with SCI, its
contributions may only be barely tapped. Part two discusses intriguing
potentials that biofeedback may yet have to offer.
Adapted from article appearing in June 2007 Paraplegia News (For subscriptions,
call 602-224-0500) or go to
http://www.pvamagazines.com/pnnews/) .
TOP
